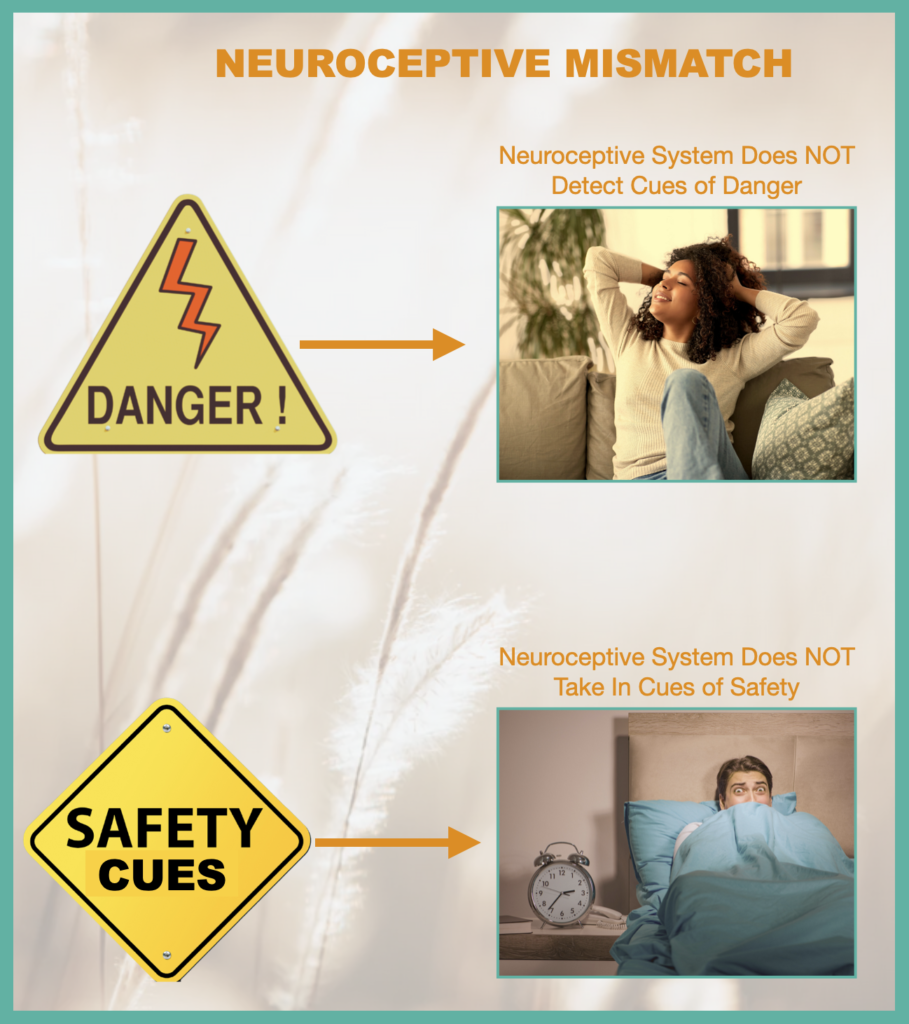
Heart-rate and blood pressure elevated; chest breathing; increased muscle tension; eyes dry; eyelids tense; frontal cortex may or may not be accessible.
 |  |
Deer in the headlights; very fast heart-rate; blood pressure significantly high; eyes very dry; may be hyperventilation; frontal cortex likely inaccessible.

Immobilized, shut down, and withdrawn; fatigued and depressed; inability to motivate; slow/delayed reactions; very low heart rate; blood pressure low; eyelids drooping; fixed gaze; may be too dissociated to feel anything; contact with self & others impossible; frontal cortex is inaccessible.
 |  |